Assistive Technology for people with amyotrophic
lateral sclerosis in Japan
: present status, analysis of problem and proposal for the future
Takuro Hatakeyama, Yokohama Rehabilitation
Center, Japan
Akira Okamoto, Ricoh Co., Ltd., Japan
Kazuo Kamata, Faculty of Engineering, Utsunomiya University,
Japan
Masao Kasuga, Faculty of Engineering, Utsunomiya University,
Japan
Corresponding author. e-mail: takuro.hatakeyama@nifty.com
Abstract:
People with severe physical disabilities such as amyotrophic
lateral sclerosis (ALS) with respirators have great difficulty
in communicating with others and expressing even their most basic
intentions and tend to be bedridden. Excellent communication
aids for such people have been developed. However, just offering
technical support is not enough for maintaining their quality
of life (QOL). Broad consideration from the areas of medicine
psychology, social science, and technology etc. is required.
In this paper, some considerations of the assistive aids for
such people are described based on ten years experience with
advanced rehabilitation services in Yokohama City, Japan. The
concept of I-world, You-world and They-world are introduced and
applied for the investigation of the client's needs and the future
direction of the service. It is our belief that through the use
of the appropriate assistive aids, people with severe physical
disabilities can return to a relatively normalized social life,
i.e. life in They-world.
Keywords:
Amyotrophic lateral sclerosis;
Assistive technology; Assistive aids; Supply system; End-user;
Needs analysis
1. Introduction
The progress of medical technology over the years has made it
possible to prolong the life span of people with amyotrophic
lateral sclerosis (ALS) using respirators. However, today in
Japan, many people with ALS still remain bedridden. On the other
hand, in recent years in Japan, there is an increasing trend
to extend the use of assistive technology to people with ALS.
As a result the quality of life for people with ALS is gradually
improving. During the past ten years, we have not only provided
assistive aids on the market to many people with ALS in Yokohama
City but also developed original assistive aids to meet client's
need [1][2][3] [4][5][6] and as a result have gained much valuable
experience. It is true that ALS patients have one of the most
severe physically limiting conditions, however we discovered
that by using assistive aids, their daily life was enhanced and
they discovered new joy and hope.
The purposes of this study are;
(1) To clarify the status and problems of people with ALS in
Japan,
(2) To define the concept of communication for people with ALS,
(3) To analyze the circumstances of providing assistive aids
through the image of I-world, You-world and They-world (explained
later),
(4) To introduce a case study,
(5) To examine a contribution to sufficient daily life through
utilizing assistive aids,
and (6) To discuss future directions.
2. Status and problem for people with ALS in Japan
In former days in Japan, almost all patients
with ALS using a respirator were required to be residents in
a hospital. Some of these patients had artificial respirators
installed without proper information or without the correct prognosis
from medical staff. As a result the situation of many people
with ALS was just to lie in bed all day wasting time with nothing
to do, without even a nurse call aid.
One of the reasons behind these problems is that in former days,
most neurologists had no relationship with staff working in the
field of rehabilitation. Such a situation still exists in some
parts of Japan. However at the present time, the number of such
people who are living at home as long as possible is gradually
increasing. When a person with ALS is living at home, the principal
person in charge of care is normally a family member, often the
personユs spouse. In this situation
a great deal of physical and mental load rests with the family.
Living at home rather than in a hospital is normally better for
the patient, however from the point of view of independence the
situation remains the same. Such patients have severe communication
difficulties and have almost nothing to do to occupy their time.
A big problem experienced by ALS patients is a sudden change
of the condition of the disease. This is not only traumatic for
the patient but also for the care staff in their attempts to
keep pace with the changes. Another difficulty is the problems
of trying to provide incentive to clients who are suffering from
the effects of medicine. Japan lags far behind in public support
systems for people living at home with ALS and there are still
some regions in Japan where suppliers and consultants of assistive
aids are in short supply or even non-existent. Information regarding
assistive aids for people with ALS is insufficient. In addition,
national assistive aid subsidies for people with ALS only covers
communication aids. On the other hand, much assistance comes
from the activities of non-governmental organizations, such as
the ALS Society of Japan. Some big problems still remain though
as to how to improve the situations for patients and family.
3. What is Communication for people with ALS?
Considering human society, we have not
only oneユs own world but also the
world of person-to-person, person-to-people and person-to-nature
/ animals. Professor Yutaka Sayeki [7] named the above I-world,
You-world and They-world. These three worlds are very important
for human beings. However, most people with ALS can access the
You-world little or not at all. By utilizing assistive aids,
there is some possibility of expanding the world of people with
ALS as far as the They-world. Figure 1 shows the concept of communication
in the broad sense. At this point it should be made clear that
I-world means the client's self, You-world means a family and
familiar environmental equipment such as television, audio unit,
personal computer and so on. They-world means a society, which
includes people such as friends, strangers, nature and animals.
The improvement of a client's quality of life is exactly what
we are aiming at. Therefore, we should consider how the people
with ALS interact with the You-world and They-world better than
now.
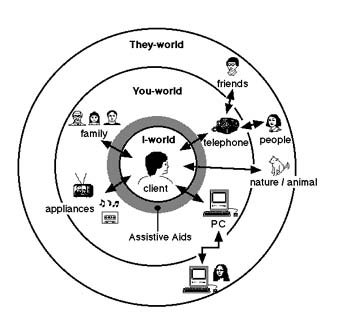
Figure 1 Communication in the broad sense on the model of Sayeki, Y. [7]
4. Proposal of new categorization of the sate of ALS client's daily living
4.1. Clients and assistive aids
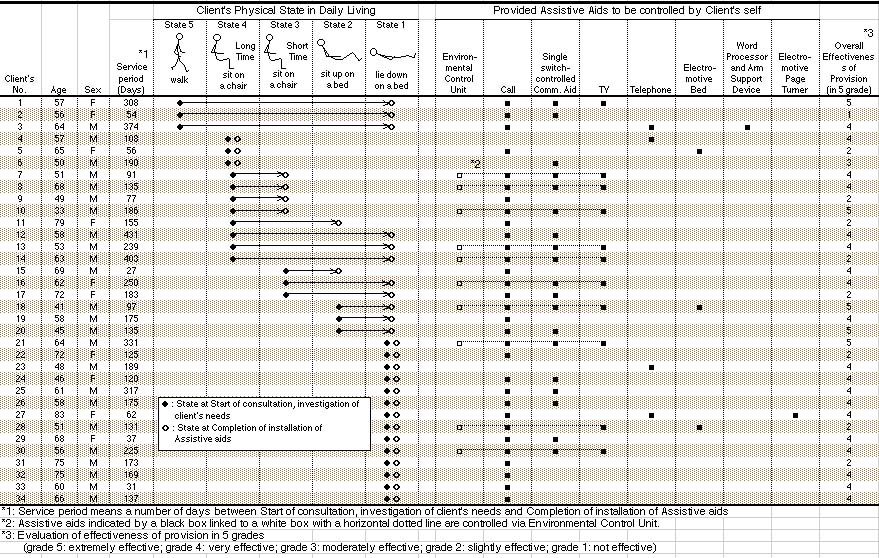
During the past 10 years, we have provided
a total of 80 assistive aids for 34 clients with ALS in Yokohama
City. Table 1 shows the situation of the provision of assistive
aids. The age of clients ranges from 33 to 83 years old, with
a mean of 59.7 years old. Among these clients 71% of them are
male.
Service period means the number of days between Start of consultation,
investigation of client's needs and Completion of installation
of assistive aids, varied from a maximum of 14.4 months, to a
minimum of 0.9 months, with an average of 5.8 months.
ICIDH-2 (The International Classification of Impairment, Activities,
and Participation) [8] is known as categorization methods. In
Japan, however, the usual evaluation method for people with ALS
is based only upon physical factors. However the data from this
evaluation method will rarely give us any hints regarding the
appropriate assistive aids for clients.
Therefore, the authors would like to propose 5 criteria to categorize
the state of the clients, considering not only their physical
factor but also their principal place of daily life. State 5
means the client is able to walk with or without a walking aid.
State 4 means the client is able to sit on a chair for a considerable
length of time (more than 3 hours). State 3 means the client
is able to sit on a chair for a shorter period of time (3 hours
and under). State 2 means the client is able to sit up in bed
for a certain time (more than 30 minutes). State 1 means the
client has to lie in bed all day. In general, clients in State
1 category almost always have to use a respirator.
Regarding start of consultation and investigation of client's
needs, a half of all clients were in early states (state 5,4),
the remaining clients were in more progressed states (state 3,
2, 1). Regarding completion of installation of assistive aids,
approximately 80% of all clients were in very progressed states
(state 2,1).
When investigating the effectiveness of assistive aids for each
client, the team responsible consists of a medical doctor, physical
therapist, occupational therapist, social worker and engineer.
This team took several points into account, some of which included
the client's and family's physical and mental factors, and ranked
the overall effectiveness (i.e. efficiency, satisfaction etc.)
of the assistive aid provided using a 5-grade evaluation system.
Grade 5 is Extremely effective, Grade 4 is Very effective, Grade
3 is Moderately effective, Grade 2 is Slightly effective and
Grade 1 is Not effective. For approximately 70% of all clients,
the evaluation was Extremely or Very effective.
Table 1 Situation for provision of assistive
aids for persons with ALS in Yokohama
4.2. Analysis
For 50% of all clients the assistive aids
were supplied from the progressive state of disease (State 2
and 1). For these clients, 82% of the supplied aids were effective.
It is our opinion that the service staff should develop a relationship
with the client from as early a state as possible. The service
period tends to be prolonged as the severity of the disease worsens.
We also believe that we should provide, in a timely manner, the
most appropriate control switch for the assistive aids according
to changes in the condition of the client's disease. The Call
aids is the most important assistive aid for most clients. Call
aids are not only a lifeline for the clients but also offer a
sense of security for both the client and their family. Single
switch-controlled Communication aids were provided to nearly
half of clients, however we discovered that many of the clients
didn't utilize the communication aid effectively due to the severity
of their disease. TV is a valuable information source from the
outside world for most clients. Telephone was a great concern
for many clients, however, unfortunately it is difficult for
most clients to speak due to their disease. Some clients wanted
to control an electrically driven bed by themselves, however
such requests must be handled with care to prevent disconnecting
the tube from a respirator.
Reading books and magazines is also a great concern for most
clients, however the number of clients using reading aids is
very low. The reason is simply due to the fact that Page turner
is very expensive in Japan, and government subsidies at the present
time do not yet include assistive aid.
Every assistive aid except TV and Telephone are mainly aids for
accessing to You-world (see Section 4). We realized that although
almost all of the clients just manage to access to You-world,
only a few clients could access to They-world.
At the present time, most of the assistive aids used by Japanese
ALS clients are made in Japan, In the future however, the authors
believe that it will be possible to utilize more high quality
products manufactured overseas, if they are more adaptable to
solving issues which exist locally, such as difference in life
style and language. These products should also be able to provide
the benefits of reasonable cost, supply stability and maintenance.
5. A case study of Mr. T with ALS
5.1. Client's profile
In our home visiting service, we have been working with a 64-year-old Mr. T (the client is No. 21 in Table 1) with ALS in an attempt to maximize his communication ability [4]. Mr. T has been on a respirator. His residual hand function allows him to generate slight movements of his right index finger. Owing to his high cognitive function and communication needs, an environmental control unit and a personal computer based Communication Aid were provided for him. The Environmental Control Unit enables him to activate the Call, control the TV set, and operate the communication aid by operating a single switch. He had been actively utilizing these assistive aids for the past 5 years.
5.2. A scene from one day's morning
Here is a scene from one morning a few
years ago: Every morning he wakes up at 6:00. His wife is still
asleep due to the previous day's rather heavy routine that is
necessary for taking care of him. He turns on the environmental
control unit by touching the fingertip switch. Then to watch
a 30-minute news program, he turns on the TV and selects the
channel by touching the switch several times. When the news is
over he turns off the TV and turns to his PC to write a story
using word processing software. He works for one hour. Then he
stores the story and turns off the PC. He turns on the TV again
to watch a morning show. At around 7:30, his wife comes into
his room to say Good morning!.
Some of readers might think it would be much easier to ask an
attendant to control these appliances, but being able to manipulate
these appliances made Mr. T realize that he could still manage
part of his life independently. This was essential for him to
sustain his dignity and maintain a reasonable quality of life.
It made him feel alive and this feeling was the source of his
motivation to keep going. After several months using the word
processor, he completed a story about his battle with ALS. Unfortunately
his physical function had declined and he could no longer move
his index finger. To compensate, a new input device utilizing
eyebrow movement was installed. He still maintains his life style
by managing some of his daily activities independently.
5.3. What did we learn from him?
The key factor in the successful provision of assistive aids is the integration of environmental control and communication function. In this client his ability to manipulate equipment around him through the environmental control unit was more meaningful for him than we had previously thought. Being able to manipulate his environment by himself not only enabled him to maintain a partially independent life style but also provided him with a feeling of well being and a sense of freedom that one feels when one is in control. Therefore, in initiation of an act, both communication and environmental control have equal value. Moreover, these feelings were the source of motivation to keep him going and assure him of inner peace, and emotional and spiritual stability, which are the foundations of his life. We believe that this aid was a major factor in the maintenance of his high quality of life during the past 5 years in spite of his very limited physical freedom.
6. Contributions to sufficient daily life of ALS clients
Figure 2 shows the conceptual rendering for extension of Activity of Daily Living by utilizing assistive aids. As the client's disease progresses, his or her own capabilities decline. In the final stages of the disease the matter of primary concern is life support. In this situation, the clients are liable to be shut in I-world. By utilizing appropriate assistive aids and human support, it is not impossible for the client to control his/her basic life (You-world), and to participate in some recreational and creative activities as well as participate in some social activities (They-world).
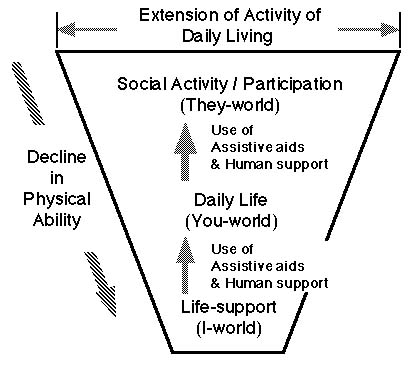
Figure 2 Conceptual rendering for extension of Activity of Daily Living
7. Discussions
Finally, we would like to discuss considerations
that we think are important in developing and providing assistive
aids to people with ALS, PMD or other severe physical disabilities.
First, there must be a precise identification of the client's
needs. It is common for clients to be unable to specify their
exact needs. If this is the case, the related staff should encourage
and help them to describe what their needs are. If the client
cannot fully identify his or her desires, clues can often be
found in the client's occupation, roles in their family, hobbies
and future dreams. Next, the staff must integrate all the information,
and clarify the client's needs and available services. The second
point is that respect for a client's self determination is essential.
In the process of developing and providing assistive aids, the
client should make any final decision. To assist in this process
of self-determination, we have to provide as many options as
possible. Encouraging self-determination usually improves the
client's sense of independence. The third point is that an appropriate
selection must be made of the level of technology utilized for
the assistive aids. The most highly advanced technology is not
necessarily the best choice. The selection has to be made through
a careful assessment of the client's physical, perceptual and
cognitive functions. We also need to realize that too much support
by assistive aids may cause the client to lose a sense of being
fully alive and his or her motivation to keep living. To minimize
this problem, any interface should be designed by utilizing the
client's residual functions appropriately. The fourth point is
that the establishment of evaluation methods for the provision
of assistive aids for the client is needed. The evaluation methods
should be considered from various viewpoints: client's and family's
physical and mental factors, client's sociability, economical
factors, and so on.
Finally, to improve the quality of client's daily living, assistive
aids that are able to help clients interact not only with You-world
but also with They-world should be further developed.
To accomplish this, extensive collaboration has to take place
with other specialists and researchers of various countries.
8. Conclusions
We newly proposed very effective categorization
that based on client's daily living rather than only physical
factors. From the view points of new categorization, we found
that even very severely progressed ALS clients can extend their
Activity of Daily Living by using appropriate assistive aids.
We are sure that from such viewpoints, we can provide much more
appropriate assistive aid and human support.
Assistive aids enrich client's quality of life and support them
in making their dreams come true. We will continue to develop
and provide assistive aids to maximize the capabilities of people
with ALS and other severe physical disabilities in order to maintain
as independent a lifestyle as possible. We will continue to discuss
an improved relationship among clients, family, nurse and assistive
aids [9].
Acknowledgements
The authors are grateful to Mr. Kevin Gallagher of The First Assistive Technology and Resource Center in Taipei, Taiwan who has been in active discussion with us regarding assistive aids, the late Mr. Toshihide Todoroki who was not only a client with PMD but also a fellow at R&D, Professor Yutaka Sayeki of University of Tokyo who gave us many suggestions about human-machine interaction, and Mr. Tadahiro Ueno and Mr. Tadashi Hatakenaka of the Yokohama Rehabilitation Center who assisted us in collecting ALS client's data.
References
[1] Hatakeyama,T., et al. (1993). Single
switch Mouse Emulator for the people with severe physical disability,
Proceedings of 9th Human Interface Symposium, 279-282. (In Japanese)
[2] Hatakeyama,T., et al. (1994). Book reading support for the
severely physically disabled, 9th Rehabilitation Engineering
Conference, 101-104. (In Japanese)
[3] Hatakeyama,T., (1995). The Development and Provision of Technical
Aids for Persons with Severe Physical Disabilities, Proceedings
of 8th ISPO World Congress (INTERNATIONAL SOCIETY FOR PROSTHETICS
AND ORTHOTICS), 187-187.
[4] Hatakeyama,T., et al. (1996). Single Switch-Controlled Electrically
driven Mirror for the people with severe physical disability,
Proceedings of 12th Human Interface Symposium, 139-144. (In Japanese)
[5] Hatakeyama,T., et al. (1996). Provision of a Communication
Device for a Homebound ALS Client, ISAAC Proceedings The 7th
Biennial Conference of the International Society for Augmentative
and Alternative Communication, 481-482.
[6] Osawa, F., et al. (1998). AAC TECHNICAL SERVICE SYSTEM AT
THE YOKOHAMA REHABILITATION CENTER, ISAAC Conference (International
Society for Augmentative and Alternative Communication), 310-311.
[7] Yutaka Sayeki. (1995). Meaning of Learning. Tokyo: Iwanami
Shoten. (In Japanese)
[8] ICIDH-2 (The International Classification of Impairment,
Activities, and Participation), URL: http://www.who.int/icidh/
[9] Hatakeyama,T., et al. (1997). Recovery of Humanity about
Nurse call, Proceedings of 12th Rehabilitation Engineering Conference,
297-300. (In Japanese)